This session immediately follows: Proceedings of the 25th National Conference; April 14, 2014 (First Plenary Session, Q & A)
We gratefully acknowledge the sponsorship of the PIH Health Family Medicine Residency Program (Whittier, California) for funding the transcription and editing of this section of the Proceedings of the Twenty-Fifth National Conference:
Mark E. Clasen, MD, Ph.D., Moderator [Dr Clasen is a Senior Fellow of the National Conferences on Primary Health Care Access]: The next panel has to do with training in primary care physicians. The panel consists of Doctors Suzanne Allen from the University of Washington Area Health Education Center in Boise, Idaho; Thomas Watson from Advocates Health System in suburbsn Chicago, and James Herman from Penn State University Medical Center. Thank you.

Suzanne Allen, MD, University of Washington (Boise, Idaho campus) [Dr Allen is the 2014 Norman B. Kahn MD National Conference Scholar]: Good morning! For those of you who are familiar with the University of Washington’s WWAMI Program (Washington, Wyoming, Alaska, Montana and Idaho),
I’m the Vice Rerent for Regional affairs so I am responsible for what we do outside Seattle across that five state region.
I live in Boise Idaho, but I work for the University of Washington.
One of the big areas that I work on in that role is actually how do we provide an adequate physician workforce for the states of the WWAMI region.
I am a member of the family medicine review committee currently. I also chair the Milestones committee for family medicine.
 I’m here, however, speaking as Suzanne Allen, not as a member of the review committee or chair of the Milestones committee.
I’m here, however, speaking as Suzanne Allen, not as a member of the review committee or chair of the Milestones committee.
Defining Competency
I will talk a little bit about competency based medical education, First, a couple of quick definitions. Competent as defined by Merriam-Webster and Oxford dictionaries is the ability to do something well, successfully or efficiently.
 If you look at the Washington State human resources website, competencies are measurable or observable knowledge, skills or abilities and behaviors that are critical to successful job performance.
If you look at the Washington State human resources website, competencies are measurable or observable knowledge, skills or abilities and behaviors that are critical to successful job performance.
Then if you look at the US Department of Education when they talk about competency based education, they state in the summary is that they are trying to transition away from being time based to becoming competency based.
 The underlying question of competency based medical education is: can you perform, and can you demonstrate mastery of a certain amount of content?
The underlying question of competency based medical education is: can you perform, and can you demonstrate mastery of a certain amount of content?
The Time Basis of Contemporary Medical Education
Where are we with competency based medical education? As we all know right now, medical education is all time based.
 We do four years of medical school, we do three to seven years of residency, depending on what specialty you’re going into; and then additional time for fellowships. So we’re really time based.
We do four years of medical school, we do three to seven years of residency, depending on what specialty you’re going into; and then additional time for fellowships. So we’re really time based.
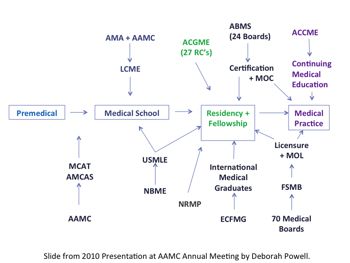
If you look at the diagram (left), which Deborah Powell put together when she was president of the AAMC, it really shows what it takes to get from being a premedical student to becoming a practicing physician and all the different entities that are involved in that process.
 It is amazing if you look at the number of different entities or accrediting bodies that are involved in the process of creating a practicing physician.
It is amazing if you look at the number of different entities or accrediting bodies that are involved in the process of creating a practicing physician.
Moving to Competency Based Medical Education
Who is working on competency based medical education right now?
For those of us who are educators, we probably all realize that it’s the Accrediting Council fo Graduate Medical Education [ACGME].
The ACGME is the independent, nonprofit organization whose mission is to improve healthcare through excellence in residency accreditation.
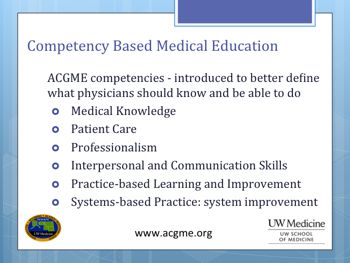
The Six Competencies
It was ACGME that started this push for competency based medical education in 1999 when they adopted the “six competencies”. (This was also called the “outcomes project”, based on the six competencies.)
ACGME realized that the outcomes (the skills possessed by graduates of residency programs) were not the skills AGCME wished to see. This was ACGME’s effort to define what should be the outcome of medical education?
The result is that now residency programs – through the accreditation process – have all their goals and objectives for their curriculum – written in competency based language.
All of the evaluations are set up in competency based language. However, the assessment processes didn’t really address the competencies, so that ACGME felt that even though evaluation processes are phrased in competency based language, the ACGME was still not getting the exact information on residency outcomes that it desired.
 The ACGME Milestones
The ACGME Milestones
That led us into the milestones, as well as the next accreditations system, which I’ will talk about briefly in a moment.
The milestones are the next step in the process of implementing the outcomes project and competency based medical education.
It was created with the goal of helping residency programs to be able to better assess their residents.
 How successful were residency programs in achieving the outcomes which they desired their graduates to have at the end of training – a competent physician who’s able to practice independently?
How successful were residency programs in achieving the outcomes which they desired their graduates to have at the end of training – a competent physician who’s able to practice independently?
The milestones are really specific benchmarks of knowledge, skills and behaviors that each resident should meet in a specified amount of time.
Some people have said that the milestones are there so that if you get out to the highest level of a milestone, then you can graduate from residency.
It’s really not the way milestones are being viewed by ACGME.
If you’re the program director, it is still your responsibility to say when someone can graduate from your program, and when that person is competent and can practice independently. The milestones are still just one tool in the process of getting there.
Restructuring the Accreditation Process
 This has been a multiyear project for the ACGME. They’ve had phase one programs and phase two programs.
This has been a multiyear project for the ACGME. They’ve had phase one programs and phase two programs.
Family medicine is a phase two program and will be implementing the milestones in July of 2014.
There were programs that did the alpha testing and programs that did the beta testing.
Some of the comments about the milestones that were made in family medicine helped them to identify and pinpoint specific areas where residents were struggling.
This should take place at an earlier point in a resident’s education than would have occurred previously.
Even for residents whom we would consider to be an excellent residents; the milestones should allow you to still give those residents some feedback on areas where they could continue to improve.
Finally, residents should be able to appreciate the feedback that they were able to get from their faculty, because it is more specific than they had received previously.
Of course, the challenge with the milestones is the process to utilize them, which must be done twice a year, takes a great deal of administrative time. This can be a huge burden to programs to adequately assess each resident’s milestones twice a year.
Continuous Accreditation
The ACGME is moving towards continuous accreditation. Where do the milestones actually fall within the next accreditation system, which, like the milestones, begins this July 2014?
Annual information will be collected. Instead of having site visits based off of whatever your accreditation cycle was previously, now every program will be visited every ten years. Before each scheduled site visit that programs will probably elect to do a self-study before the site visit.
Additionally, there may be focused site visits within the accreditation cycle, depending upon what the review committee sees in the annual data that they have been provided.
 Clinical Learning Environment Review [CLER]
Clinical Learning Environment Review [CLER]
Another important change is called the Clinical Learning Environment Review [CLER] visit, which I’m going to talk about briefly. At present, ACGME is saying that CLER visits will not affect a program’s accreditation, but certainly it is something to which attention will be paid.
What are the annual data to be collected?
The Accreditation Data System [ADS] will have 33 questions that every program has to answer. These questions will be updated every year.
 A resident survey and a faculty survey will be done done every year, and the milestone data reported twice a year, Additionally, board certification data will be provided from each specific specialty board to that specialty’s review committees
A resident survey and a faculty survey will be done done every year, and the milestone data reported twice a year, Additionally, board certification data will be provided from each specific specialty board to that specialty’s review committees
Clinical experience in family medicine accreditation data collected will include the number of patients that residents are seeing in the outpatient setting? For the surgical specialties, the data will include the case lots from the surgeries the residents have performed.
Key quality data, patient safety data, and evidence of scholarly activity both by the faculty members and the residents will be collected. Finally, the institutional support will be asssesed. Is the institution doing o. k. financially? What has the leadership been for the institution? Has there been a huge amount of faculty turnover? How is the institution supporting graduate medical education?
THe CLER visits will have have six specific areas that they will focus on; patient safety, quality improvement, how residents are supervised, transitions in care, duty hours or fatigue management, and professionalism.
 When you have a CLER visit, there will be five questions asked. How is the institution’s infrastructure designed to address those six focus areas? How engaged is the graduate medical education (GME) leadership? Similarly, how engaged are the residents and fellows?
When you have a CLER visit, there will be five questions asked. How is the institution’s infrastructure designed to address those six focus areas? How engaged is the graduate medical education (GME) leadership? Similarly, how engaged are the residents and fellows?
How is the success of the institutional efforts measured? What areas have been identified for improvement.
These CLER visits have been envisioned to look closely at how is the residents’ GME is incorporated into the institution’s patient care and patient safety procedures?
We certainly know that residents provide a considerable part of the patient care in any inpatient setting. Without them it would be difficult for many of our hospitals or institutions to provide patient care, yet residents frequently are not included in any of the quality improvement or patient safety type committees.
That is what the CLER visits are designed to do. First, to help train the residents in how they can impact the system so as to improve patient care and patient safety, and participate in quality improvement. This process is expected to lead to the institutions realizing that the residents and fellows can provide valuable information in making these improvements.
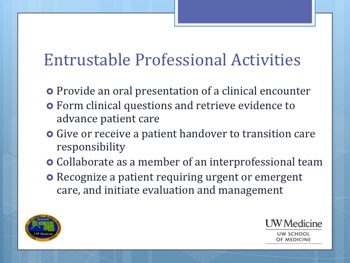
Entrustable Professional Activities [EPA]
 Returning to the subject of competencies, which I touched on a little bit in my remarks about the next accreditation cycle, I want to describe the entrustable professional activities (EPAs).
Returning to the subject of competencies, which I touched on a little bit in my remarks about the next accreditation cycle, I want to describe the entrustable professional activities (EPAs).
These are different from the milestones discussed above. They are also different from the competencies.
EPAs, as they are called, define the essence of what a professional must do. EPAs describe the work that defines each specific discipline.
 A lot of work has been done on the EPAs within the discipline of Pediatrics.
A lot of work has been done on the EPAs within the discipline of Pediatrics.
In fact, Pediatrics included EPAs as part of their milestones and as part of their competencies.
If you think of milestones as being things defined behavior, skills, knowledge that we can look at and check a box saying “you’ve accomplished that particular competency or milestone”, then you EPA being that thing where you say, “yes, you can trust this person to perform this skill”.
 Pediatrics has already included their defined EPAs into their milestones. Internal medicine is working on doing the same.
Pediatrics has already included their defined EPAs into their milestones. Internal medicine is working on doing the same.
There is a committee of the Society of Teachers of Family Medicine that is currently working on EPAs for family medicine.
I think we may see in the future that EPAs will become a next step along the continuum of the competencies that we’ve been working on.
LCEM Competencies in Medical Education
So where else do we see competencies in medical education being developed? The Liaison Council of Medical Education (LCME) requires that all medical schools have educational objectives. Those educational objectives have to be based in outcomes that are “valued” by the profession.
Currently, LCME doesn’t use the ACGME competencies at all. There has been work being done by AAMC, which is one of the two partners that make up the LCME, the other partner being the AMA.
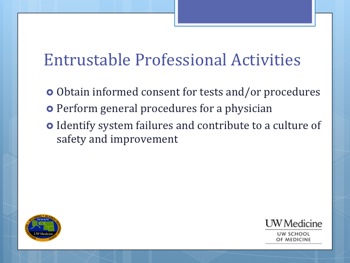
The AAMC has been doing some work on EPAs that are essentially for medical students. There’s a link here that you can look at the document that I think is somewhat helpful as it gives specific information about the 13 EPAs they’ve established so far..
These are just the EPAs that they’ve come up with; I’m not going to spend time talking about any of them. They are the general things that you might imagine you would want every medical student to be able to do before they graduated from medical school and entered any residency program..
There still needs to be work done to see how these work within medical schools. There are a number of schools who have volunteered to adopt the proposed EPAs on a trial basis. It is a little unclear how thes EPAs will evolve after that.
American Board of Medical Specialties (ABMS) Competencies
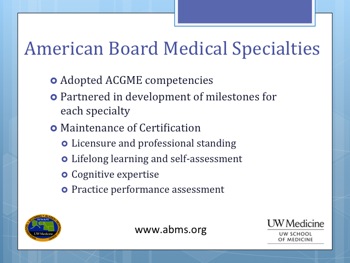 The American Board of Medical Specialties has adopted the six ACGME competencies. ABMS has been partners with the ACGME in the development of milestones.
The American Board of Medical Specialties has adopted the six ACGME competencies. ABMS has been partners with the ACGME in the development of milestones.
The ABMS established milestones for the maintenance of certification.
First, a physician should have a valid unrestricted license to practice medicine.
The physician should participate in continuing education and self-assessment modules.
To assure a physician’s cognitive expertise, most of us will have to take an exam every 10 years. Practice performance – the physician’s clinical skills are assessed also.
Concluding Remarks
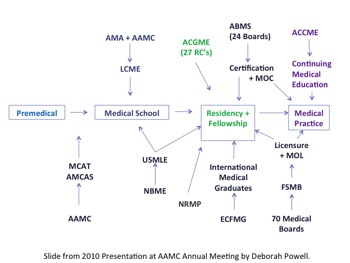 Let’s return to the diagramming of the process by which a premedical student becomes a practicing physician, noting all the different entities and accrediting bodies that are a part of that process.
Let’s return to the diagramming of the process by which a premedical student becomes a practicing physician, noting all the different entities and accrediting bodies that are a part of that process.
Certainly the most of the work being done around competency education is being done at the ACGME level now; a little work starting on the LCME level.
ABMS is working on it. So does this mean at some point in time we’re gonna be able to go just a competency based training, as opposed to “length of time in training”? I think that’s a great question for discussion. I’ll end my presentation there and turn the microphone over to I think Dr. Hansen, who is speaking next.
Thank you.
This section is followed by: Proceedings of the 25th National Conference: April 14, 2014 – Second Plenary Session, Part 2 (Hansen)